Had practical lesson in Arrhythmia-ICU today. Dr. Valek kicked off the session with some ECGs for us to interpret. I am quite satisfied with myself for not knowing 'only' 4 of them, LOL. I must really thank Dr. Thaller :)
I was quite amazed by the multiple ECGs of a same patient with WPW syndrome.
Something I read about WPW syndrome but did not realised its importance:
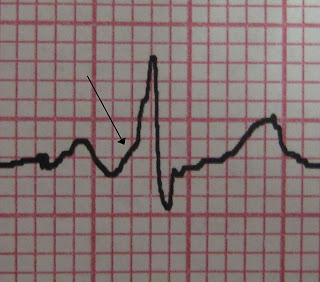 -if there is short PR interval, wide ORS with delta wave but patient doesn't have paroxysmal tachycardia, the patient has only preexcitation and this is called WPW pattern.
-if there is short PR interval, wide ORS with delta wave but patient doesn't have paroxysmal tachycardia, the patient has only preexcitation and this is called WPW pattern.
-if there is WPW pattern(as mentioned above) and patient has history of paroxysmal tachycardia, it is then only called WPW syndrome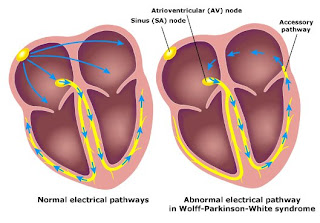 -the most common arrhythmia in WPW syndrome is Atrioventricular Reentrant Tachycardia(AVRT)
-the most common arrhythmia in WPW syndrome is Atrioventricular Reentrant Tachycardia(AVRT)
-there are two forms of AVRT: orhtodromic AVRT and antidromic AVRT (depending on how the impulse goes in the reentrant circuit)
-Vagal maneuvre can be used to terminate AVRT as it transiently blocks AVN
-Atrial Fibrillation and Atrial Flutter can occur too
-Rx: antiarrhythmics
-Do not use calcium channel blocker, digoxin or beta blocker!!
-iv procainamide for AF and AFL in patient with bypass tract. Electrical cardioversion can be considered
-radiofrequency cathether ablation (95% success rate)*Study Lown-Ganong-Levine Syndrome too!


